

Background
Since the FDA approval of clofarabine for the treatment of relapsed or refractory acute lymphoblastic leukemia (ALL) at childhood, several studies have been launched which put clofarabine under scrutiny in combination with other cytostatic drugs as second or third line therapy. As a novel treatment-strategy we introduced the combination of clofarabine with pegylated asparaginase (PEG-ASP) in a randomized fashion in comparison to the standard consolidation course with high dose cytarabine (Hidac) combined with PEG-ASP into the frontline management of ALL within the CoALL 08-09 protocol. The primary objective of the study was to compare the MRD based assessment of the cytotoxic efficacy of the randomized courses in pediatric ALL.
Patients and methods
CoALL 08-09 was an open, interventional, multi-center, prospective, and randomized clinical trial for patients with newly diagnosed ALL. In March 2010 the trial had been opened for enrollment of patients under 18 years with confirmed diagnosis of acute B- or T-cell precursor leukemia. After a stratified phase I/II, in which patients with high-risk features and high post-induction MRD received the combination of clofarabine and PEG-ASP, the randomized trial started in November 2013. All patients with a measurable MRD at the end of induction (EOI), as measured by RQ-PCR according to EURO-MRD guidelines, were eligible for randomization to receive either the combination of clofarabine 5 x 40 mg/m2 or high dose cytarabine (HIDAC) 4 x 3g/m2 bothin combination with PEG-ASP 2.500 IU/m2 at the beginning of the consolidation phase. Until December 2019 303 study patients were randomized allocating 151 patients towards the clofarabine and 152 patients to the HIDAC arm. Patient characteristics and MRD burden prior to this treatment element were highly comparable.
Results
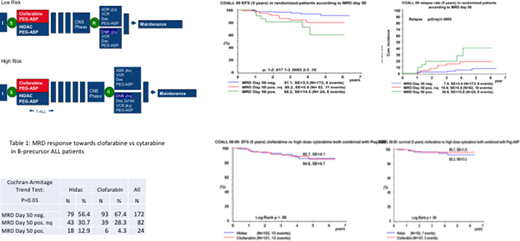
The reduction of minimal residual disease was significantly more profound after clofarabine compared to cytarabine (p(Cochran-Armitage)=.01 for BCP-ALL with 93 vs 79 patients reaching MRD negativity (Table 1). MRD status of BCP-ALL after the first randomized consolidation block (day 50) was of prognostic relevance with a statistically significant impact on EFS and relapse rate (Fig. 2a). However, no difference in outcome regarding the event-free and overall survival between the randomized arms was observed (5-year EFS: Clofarabine 85.7, SE=4.1 vs Hidac 84.8, SE=4.7 (p=.96) and OS: 95.7, SE=1.9 vs 92.2, SE=3.2(p=.59) Fig. 2b). This finding was recapitulated independent of gender, age, WBC count at diagnosis, ETV6-RUNX 1 translocation, immunophenotype or overall risk strata). Results for T-ALL patients are in the same range but because of small numbers not statistically significant. No differences in the incidence of severe or persistent toxicity btween randomized treatment elements as well as in the subsequent treatment realization were registered.
Conclusion
Clofarabine combined with PEG-asparaginase is highly effective and well tolerated in the frontline treatment of ALL. Although the prognostic impact of MRD is still discernible in early consolidation, the greater cytotoxic efficacy of clofarabine reflected by a more frequent eradication of MRD, did not translate into an apparent improvement of outcome likely due to a lack of power in the comparative analysis of randomized patients.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal